|
| Image 1: Right in the starting block is where heart health begins... and on the finish line of a marathon race probably is where heart health ends (if not much earlier) |
I think it is unnecessary to pose this question again, but in case you missed the innumerable blogposts, where I asked you whether you would rather like to look like an ultra-endurance runner or like a sprinter - here you go:
Whose physique would you rather want to have? The sinewy physique of Haile Gebrsellasie or the muscled physique of Usain Bolt and co? I assume in most cases this question is unnecessary... but
what if you are sick, obese or even have a heart failure? Obviously you cannot train like a sprinter, then... can you? Yes, you can - at least within your personal physiological limitations! In view of the results of a recent study from the
KG Jebsen Center of Exercise Medicine at the
Norwegian University in Trondheim, Norway, aerobic interval training would even be the
healthier choice
(Moholdt. 2011)!
For their study Trine Moholdt and her colleagues recruited 107 patients who had been hospitalized for myocardial infarction 2-12 weeks before the study and randomly assigned them to
usual care rehabilitation or an aerobic interval training performed. In the course of the
12 week study period the exercise protocol was performed thrice a week. Two sessions were supervised, the other one had to be performed at home.
- usual care rehabilitation program - the standard program comprised 60 minutes of aerobic exercises performed to music; the sessions were lead by a physiotherapists, and after a 10-minute warm-up, the patients did aerobic exercises like walking, jogging, lunges and squats for 35 minutes, which were followed by a 5-minute cool-down with stretching and relaxation exercises.
- aerobic interval training - the total session time of the interval training was 38 minutes; it consisted of an 8-minute warm-up, followed by 4x4-minute intervals at 85–95% of the maximum heart rate (monitored by heart rate monitor), with active rest of 3 minutes of walking at 70% of maximum heart in between the intervals; the exercise session was terminated with a 5-minutes cool-down.
In view of the still
commonly held believe that interval training could easily become (over-)exerting, quite a few medical practitioners, would probably shake their heads over the "irresponsibility of [their] Norwegian collegues -
how dare those idiots put ailing cardiac patients on such an tortorous exercise regimen" ... I think I won't have to continue,
you know the whole litany... and if you, just like me cannot stand that anymore, and your own (your father's, mother's, grandpa's or grandma's) doctor is one of those, take the following data, print it and use it to shut him up.
 |
| Figure 1: Improvements in VO2Max, peak heart rate, respiratory exchange rate at peak heart rate and heart rate recovery in cardiac patients after 12 weeks on the usual care rehabiliation program or an intense aerobic interval training (data calculated based on Moholdt. 2011) |
Obviously,
the poor cardiac patients did not only survive the "torture", their hearts even thrived on it. The increase in peak oxygen uptake (VO2Max), the standard measure of aerobic performance, was 2.7x higher in the interval group than in the patients who did the usual 60-minutes reha-sessions (cf. figure 1). For the other parameters the differences were not statistically significant after analysis for initial randomization:
Flow-mediated vasodilatation, both non-normalised and normalised to shear stimulus, increased significantly after exercise training in both groups [...] Quality of life increased significantly after exercise training (between-group differences, not significant)
If we look at the blood parameters, however, we do yet see some interesting differences, even your medical practitioner could not argue away:
 |
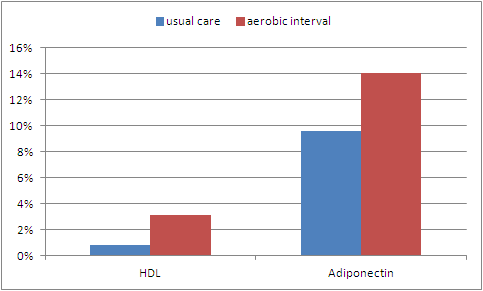
| Figure 2: Changes in high density lipoprotein and adiponectin in cardiac patients after 12 weeks on the usual care rehabiliation program or an intense aerobic interval training (data calculated based on Moholdt. 2011) |
While the changes in
triglycerides, CRP, ferritin, haemoglobin, and
glucose were - within their respective standard-deviations - identical in both groups, there was a
marginal but statistically significant greater improvement in high density lipoprotein (HDL) levels (a statistician would say there was an improvement in the interval group, while there was none / no statistically significant one in the reha-group) in the interval group. While this would indicate a lower risk of future (recurrent) heart disease, the accompanying increase in adiponectin would suggest that the interval training group either had already or were about to lose more body fat than their endurance trained peers.
Unfortunately, the body composition of the patients was not tracked in the study, so this leaves us with
the "surprising" benefits of intense interval training for the hearts of patients with prior myocardial infarction as the main result of a study some medical practitioners would probably not even have dared conducting.