 |
| Image 1: Cobalt - certainly not what you would expect to see at a health food store or pharmacy; with Kawakami et al.'s study this may change in the future (img Alchemist-hp) |
"We are living in a toxic world!" - you have probably heard or read this sentence more than once and while I cannot deny that the environmental load of, among others, heavy metals appears to be increasing, I can however tell you that, according to a recent study from scientists from the
Tukushima Bunri University in Japan,
exposure to some of those heavy metals produces quite unexpected results in a rodent model of the metabolic syndrome and in lean controls. Instead of making them gain weight even more rapidly, the "toxic" (maybe we will have to reconsider that, just as we did in the case of chromium) heavy metal cobalt did not only reduce the weight of the white adipose tissue of the rodents, it increased leptin, adiponectin, and HDL-cholesterol, as well, and thusly "may have a preventive role in obesity-related diseases" (
Kawakami. 2011)
This is certainly the 1001st time I am writing this, but I cannot emphasize often enough that the "high fat diet" researchers use in their studies has (in most cases) nothing to do with the Atkins or even a low-carb diet. Its main characteristic is that it is hypercaloric and high in fat and carbs. Please keep that in mind whenever you read about another study on the detrimental health effects of "high fat diets".
For 24days Kawakami et al. fed a group of seven-weeks-old male mice either a standard diet with 357.6kcal/100g or a
hypercaloric (cf. red box above) high fat diet (HFD), where the latter induced obesity and dislepidemia within 2 weeks. After this initial phase, i.e. when the HFD mice were already obese and metabolically deranged, the scientists injected the animals with
Sodium Arsenite (NaAsO2: 1.0 mg/kg bw),
Mercuric Chloride (HgCl2: 1.0 mg/kg bw),
Manganese Chloride (MnCl2: 5.0 mg/kg bw), Cobalt Chloride (CoCl2: 0, 1.3, 5.0, 7.5 mg/kg bw) or saline (control).
 |
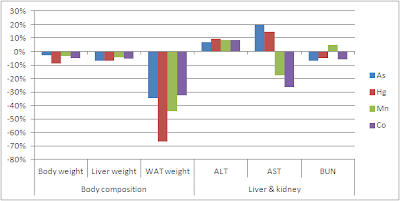
| Figure 1: Modulatory effects of 10 days of heavy metal injection in mice on a high fat diet; values expressed as changes relative to animals on a normal diet (data calculated based on Kawakami. 2011) |
Now, if you look at the data in figure 1, you will notice that the administration of
Mercuric Chloride may have been most "effective" in ameliorating the HFD-induced increase in white adipose tissue (WAT) mass (HFD +70%; HgCl2 -14% vs. normal fed control), but
those "fat burning" effects went hand in hand with profound elevations of the liver enzymes AST, ALT (in this case we can safely assume that these were not coming from the muscle tissue of the animals)
and the blood urea nitrogen (BUN) levels, which indicate deteriorations of the kidney metabolism. Manganese and cobalt, on the other hand, had negligible or even beneficial effects (compared to HFD alone) on liver and kidney health and ameliorated the weight gain to +10% and +17%, respectively.
 |
| Figure 2: Adiponectin and leptin serum levels and mRNA expression in mice after 10 days on a high fat diet with simulatenous injection of mercury or cobalt; data expressed relative to normal fed control (calculated based on Kawakami. 2011) |
What is particularly interesting about cobalt, though, is that it did not simply starve out the adipose tissue by poisoning it (like that was probably the case for mercury), but triggered exactly those metabolic adaptations scientists have been trying to provoke with drugs for years now:
elevations in adiponectin and
leptin (cf. figure 2), the two adipokines, researchers currently believe to be essential for successful weight loss / maintenance.
 |
| Figure 3: pAMPK/AMPK ratio after injection of different dosages of Cobalt chloride (calculated based on Kawakami. 2011) |
In a follow up experiment, the scientists, also found that
cobalt dose-dependently increases AMPK phosphorylation (for more on AMPK, I would like to refer you to the
Intermittent Thoughts series) in white adipose tissue (WAT), muscle and liver of the animals (cf. figure 3). Of the three tested dosages, administration of 5mg/kg CoCl2 per day resulted in the most beneficial AMPK response, while with the maximal dose of 7.5mg/kg the negative / toxic effects appear to prevail (another of these bell-shaped dose-response curves, I guess).
 |
| Figure 4: Glucose tolerance test in mice on high fat diet with or without cobalt injections compared to mice on standard diet (control); values in mg/dl (data adapted from Kawakami. 2011) |
Now, you are probably asking yourselves: "So what's the catch?". A brief look at figure 4 tells you that is ain't glucose intolerance, as the cobalt treated animals had the exact same response to the glucose tolerance test, as the mice on the normal diet - in other words:
cobalt completely reversed the HFD induced glucose intolerance, and it did so not only without negative effects on blood lipids, but in the presence of a
profound elevation of HDL levels and a reduction in LDL levels (cf. figure 5).
 |
| Figure 5: Relative (to normal fed control) changes in blood lipid in mice on a high fat diet with or without heavy metal injections (calculated based on Kawakami. 2011) |
And as if that was not enough, the cobalt injections also eradicated the iincreases in free fatty acids and ameliorated the increase in triglycerides.
From the lab to the bedside? Last but not least, and I hardly dare showing you this graph, because I would expect that some of you will already be googling a source of injectable cobalt
(which would be plain out stupid, before any reliable safety data and confirmation of these results in controlled human trials are available), cobalt had almost identical effects when it was injected to the mice on the normal diet.
 |
| Figure 6: Relative changes in body composition and liver and kidney parameters due to heavy metal injection in non-obese mice on a standard diet (calculated based on Kawakami. 2011) |
As figure 6 goes to show the
mice lost 33% of their white adipose tissue and liver, as well as kidney function did not take a beating (HDL stayed the same, LDL decreased by -1%). Whether we will see a obesity or even just a weight-loss drug based on cobalt in the near future, does yet still seem questionable. In view of the fact that the number of "bad things" (
cobalt is in fact an essential nutrient as it is the
active center of
vitamin B12 = cobal-amin) that have unexpectedly positive health effects is increasing day by day, we do yet obviously have to ask ourselves, whether there may be some major flaws in our current understanding of how our body works and how it deals and is effected by "toxins", oxidants and co.






