 |
| Image 1: I guess after the publication of his latest study, Mr. Bhasin will have a bad standing with the pharma reps from GlaxoSmithKline & Co ;-) |
The "Big T" as in "Testosterone" or as in "Taboo"?
As an MD you are not supposed to ask these questions... you are not even supposed to put your male patients on TRT. What you are yet supposed to do is to believe in all the fairy tales the reps from pharmaceutical industry are serving you up with: "Testosterone replacement is dangerous! It is irresponsible [blablabla...], but if it really is necessary, make sure you also prescribe our newest 5-alpha reductase inhibitor [...]"... hold on, I wanted to refrain from the whimpering, so let's get to a real man, who does the balls to ask these questions and the boldness to do human trials to answer them: Shalender Bhasin!
 |
| Figure 1: Dose response relationship of muscle gain (in kg) per mg of testosterone enanthate; the white line indicates a dose that would probably have produce testosterone levels identical to baseline (calculated based on Bhasin. 2001) |
Testosterone + Dustasteride = More Muscle and Less Prostate Growth?
In their latest study Bhasin et al. conducted an experiment that was actually pretty similar to their previous trial (Bhasin. 2012). The subjects were once more healthy, eugonodal (= normal testosterone levels) men, this time however from a broader age-range (18-50y; mean age ~40y) than in their previous trial (18-30y). The dosing protocol was identical (50, 125, 300 or 600mg/week testosterone enanthate) and even the treatment period, 20 weeks, was (I would guess) deliberately matched to that of the 2001 study on the dose-response relationship between exogenous testosterone administration and improvements in body composition (Bhasin. 2001). I have discussed in length in the previously cited blogpost. The single innovation in this study was thusly the administration go 2.5mg of the potent 5-alpha reductase inhibitor dustasteride to 70 of the 139 subjects.
 |
| Image 2: Natural DHT modulation therapy with rice, safflower & sorghum |
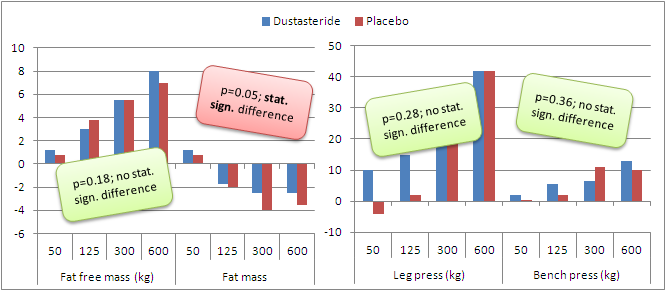 |
| Figure 2: Increases in fat free mass and fat mass, as well as leg press and bench press strength (all values in kg) after 20 weeks on different doses of testosterone enanthate (50, 125, 300, 600mg/week) with or without 2.5mg of dustasteride per day (data adapted from Bhasin. 2012) |
 |
| Table 1: Incidence of side effects in the subjects of the two study arms (adapted from Bhasin. 2012) |
"And what about my prostate and cholesterol levels?"
Although Bhasin et al. defined the effects of dustasteride administration on the "maintenance of androgen effects on sexual function, hematocrit, sebum production, bone markers, and lipid levels" as their secondary outcomes and winked at the potential increases in prostate size, they did not make themselves even more vulnerable to the attacks from the anti-TRT crowd by simply ignoring this issue and did measure the prostate sizes before and after the 20-week intervention by the means of magnetic resonance imaging and found that...
[...c]hanges in prostate volume and PSA level were not significantly related to either testosterone dose or concentration, and did not differ significantly between the placebo and dutasteride groups. The dose-adjustment mean difference in change in PSA level between participants assigned to placebo and participants assigned to dutasteride was 0.13ng/mL (95% CI, −0.05 to 0.31 ng/mL; P = .15) and the corresponding difference in changes in prostate volume was 0.91 cm³ (−0.44 to 2.25 cm³; P = .19).The incidence of acne (sebum production) was identical (25 subjects in both groups) and the "acne scores did not differ between groups." Lastly, the levels of "hemoglobin and hematocrit increased dose dependently in the placebo and dutasteride groups" and did "not differ significantly between the groups". In view of the fact that the dose-dependent decreases in total and HDL were also identical between the groups and neither the serum NTx (collagen-type I N-telopeptides), nor the osteocalcin levels were hampered or promoted by the addition of dustasteride to the TRT regimen, there appears to be no reason for an otherwise healthy man to take a drug, which in and out of itself can produce serious and in rare cases even permanent side-effects (cf. "Finasteride Kills Male Libido Permanently").
Don't Base Your Judgement on Hearsay and the Results of Others - Get Labs Done!
That being said, there are certainly cases, where the enzymatic cascade is messed up and the more or less uncontrolled over-production of dihydrotestosterone would not only compromise the beneficial of injectable testosterone, but pose a serious health risk. Especially for those of you who are on TRT for medical reasons (and by the way, there is no such thing as a "trenbolone deficiency", bros ;-), it would thusly be prudent to base your decision for or against an 5-ar inhibitor on your individual serum levels... and, regardless of whether you decide to take or to decline your MD's offer, you better make sure that your testosterone is not shoveled to the other, the estrogenic side of the hormonal divide!