 |
| Image 1: Are you taking copious amounts of synthyroid (levothyroxin, T4), already, and feel as if your hypothyroidism became rather worse than better? Does Your Dr tell you that your TSH is fine and you should just exercise more and eat less to stop gaining weight like mad? Than this post is for you! |
"Nurse, send the patient home and show me his lab report!"
The real-life consequences of treating lab values instead of patients and going by textbook prescriptions instead of the often debilitating symptoms of hypothyroidism which range from
- physical problems such as weight gain, constipation, constant cold, feeling of cold, blurred vision, nausea, sleepiness, low blood pressure, high cholesterol and blood glucose levels, etc. to
- psychological issues such as general cognitive decline, inability to concentrate, mental fatigue, anger, confusion and depression
 |
| Image 2: Ladies, you are lucky you got all that subcutaneous fat to absorb those lubricants and PCB laden cosmetics you are using and stash it away ... a pity it's all going to haunt you, when you want to get rid of those fatty, unaesthetic dumping grounds. |
- hexachlorobenzene (HCB), which was used as a pesticide until 1965 and was also used in the production of rubber, aluminum, and dyes and in wood preservation and is currently formed as a byproduct during the manufacture of other chemicals, mainly solvents and pesticides, and
- PCB 156, one of the members of the olychlorinated biphenyl (PCB) family of chemicals that has now been banned from industrial insulators and lubricants, because of substantial evidence of its carcinogenic and neurotoxic effects.
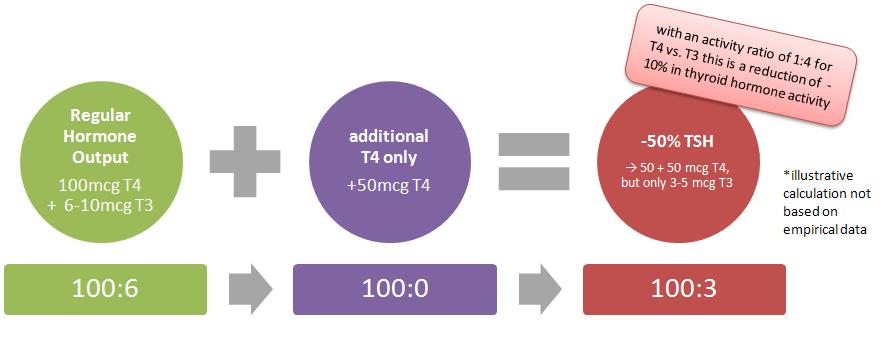 |
| Figure 1: Illustrative "calculation" of the effects of partial thyroid hormone replacement with 50mcg T4 only. |
- possible increase in conversion of T4 to rT3 and thus "anti-thyroid" activity; the latter is especially prominent in insulin resistant individuals (Ruhla. 2011) and those receiving high doses of T4 (Clur. 1986) Note: this renders the recommendation to simply up the doses of T4 to levels with partially suppressed TSH levels Ito et al. make in the initially cited study pretty much nonsensical
- lack of enzymatic conversion at the level of the target tissue and consequently even lower thyroid activity; something that is often seen in patients who have a "sluggish thyroid metabolism" anyways and receive only a partial substitution
Against this background, it stands to reason that the argument "but it works for most of my clients" you will often hear from your Dr. is of little significance for you as an individual and even a statement like "but didn't you feel better, when we initiated the treatment 2 months ago" could not just be missing the boat, altogether, but brings another commonly overlooked problem to mind: If you have been suffering from symptoms of hypothyroidism for a couple of years, you would probably feel "major improvements" if you went from a "1" as in "very bad" to a "3" as in "bad", without knowing that you may, just as the majority of the subjects in a study that's been published in The New England Journal of Medicine in 1999, feel even better if you received 12.5mcg of T3 instead of 50mcg of the T4 your Dr. has prescribed.
T4 + T3 therapy makes subjects feel better, 20/32 don't want to go back on monotherapy
The 31 hypothyroid patients who took part in the 10-week study during which the participants received in random order either their regular "T4 only" thyroid medication (e.g. 200mcg of T4) or an identically looking combination preparation in which 50mcg of the original T4 dosage had been replaced with 12.5mcg of T3 (e.g. 150mcg T4 + 12.5mcg T3). The patients, 31 women and 2 men with a mean age of 46 years and either autoimmune thyroiditis or thyroid cancer that was treated with baseline doses of 75±53 µg T4 per day (range 100-300 µg), were closely monitored during the both of the 5-week interventions and biochemical, physiologic, and psychological tests were performed at the end of each treatment period.
 |
| Figure 2: Cognitive performance and psychological well-being of the 32 subjects of the Bunevicius study assessed by standardized tests on either regular T4 only or T4 and T3 combination protocols (based on Bunevicius. 1999) |
 |
| Figure 3: Mood and physical symptoms in the 32 subjects of the Bunevicius study assessed by straight forward questionnaires with visual analogue scales - this is the "how do yo actually feel" data (based on Bunevicius. 1999) |
[w]hen asked at the end of the study whether they preferred the first or second treatment, 20 patients preferred thyroxine plus triiodothyronine, 11 had no preference, and 2 preferred thyroxine alone (P=0.001).These results were unrelated to the order of treatment and the two patients who preferred the T4 only treatment had probably ended up slightly hyperthyroid as they were complaining of feeling "slightly nervous during combined treatment" (Bunevicius. 1999). The others however emphasized that they "noticed that they were more energetic, had better concentration, and simply felt better" (ibid.) than on T4 alone.
The Bunevicius study in nuce
Protocol Reduce T4 intake by 4mcg per 1mcg of T3 you introduce; optimally reduce T4 intake by 50mcg and att 12.5mcg of T3 in.
Results Thyroid hormone levels staid in range (see table above), the +3beat/min increase in pulse rate is harmless and the non-significant drop of 6 and 2pts in systolic and diastolic blood pressure is nothing to speak of.
| T4 | T4+T3 | |
| TSH (µU/ml) | 0.8 | 0.5 |
| TSH = 0* | 7 | 5 |
| T4 (µg/dl) | 15.2 | 11.3 |
| T3 (ng/dl) | 87 | 117 |
Table 1: Serum levels of selected hormones and *# of patients with serum TSH <0.05µU/ml
Side Effects Two subjects felt slightly agitated on T4 + T3, no other side effect were reported
Useful for people who are taking high (>>50mcg) doses of T4 (only under supervision of your Dr!)
Not useful for people who don't need thyroid medication and simply suffer from low thyroid hormone due to overtraining, undereating or both (see links below).
Moreover, the notion of "just throwing in T4 and waiting for the target tissue to produce as much T3 from it as needed" is intrinsically flawed as it negates the established exogenous T3 requirements of the mammalian brain (~20% of the T3; cf. Silva. 1984), as well as the local downregulation of the T4 => T3 conversion in the brain upon exposure to elevated serum thyroxine (T4) levels (Silva. 1985), as they will occur whenever you simply "up the dosage" of levothyroxine in the false belief that this would help you to get rid of persistent symptoms of hypothyroidism. Against that background it appears to be rather the exception than the norm that you would be optimally functioning on T4 only and not end up
- still systemically hypothyroid with even lower serum T3 levels (or T3-to-rT3 ratios), than before, or
- now centrally (in the brain) hypothyroid despite "normal" or even suppressed TSH levels and adequate or high circulating thyroid hormone levels
References:
- Bunevicius R, Kazanavicius G, Zalinkevicius R, Prange AJ Jr. Effects of thyroxine as compared with thyroxine plus triiodothyronine in patients with hypothyroidism. N Engl J Med. 1999 Feb 11;340(6):424-9.
- Clur A. Reverse tri-iodothyronine as part of alpha 2 adrenergic receptors. Med Hypotheses. 1986 Nov;21(3):281-92.
- Hue O, Marcotte J, Berrigan F, Simoneau M, Doré J, Marceau P, Marceau S, Tremblay A, Teasdale N. Increased plasma levels of toxic pollutants accompanying weight loss induced by hypocaloric diet or by bariatric surgery. Obes Surg. 2006 Sep;16(9):1145-54.
- Ito M, Miyauchi A, Morita S, Kudo T, Nishihara E, Kihara M, Takamura Y, Ito Y, Kobayashi K, Miya A, Kubota S, Amino N. TSH-suppressive doses of levothyroxine are required to achieve preoperative native serum triiodothyronine levels in patients who have undergone total thyroidectomy. Eur J Endocrinol. 2012 Jun 18.
- Koury EJ, Pawlyk AC, Berrodin TJ, Smolenski CL, Nagpal S, Deecher DC. Characterization of ligands for thyroid receptor subtypes and their interactions with co-regulators. Steroids. 2009 Feb;74(2):270-6.
- Ruhla S, Arafat AM, Weickert MO, Osterhoff M, Isken F, Spranger J, Schöfl C, Pfeiffer AF, Möhlig M. T3/rT3-ratio is associated with insulin resistance independent of TSH. Horm Metab Res. 2011 Feb;43(2):130-4.
- Silva JE, Matthews PS. Production rates and turnover of triiodothyronine in rat-developing cerebral cortex and cerebellum: responses to hypothyroidism. J Clin Invest 1984;74:1035-49.
- Silva JE, Leonard JL. Regulation of rat cerebrocortical and adenohypophyseal type II 5'-deiodinase by thyroxine, triiodothyronine, and reverse triiodothyronine. Endocrinology 1985;116:1627-35.
- Tremblay A, Pelletier C, Doucet E, Imbeault P. Thermogenesis and weight loss in obese individuals: a primary association with organochlorine pollution. Int J Obes Relat Metab Disord. 2004 Jul;28(7):936-9.