 |
| As the data in the graphs at the bottom shows, only vigorous physical activity (right), yet not moderate (middle), let alone light physical activity (left) will help kids to stave off the bad visceral body fat, which increases their waist line from year to year. The photo in the background was by the way taken in 1989 on Orchard Beach, in the Bronx. If I remember correctly that's 6 years before the release of Nintendo's first "Game Boy". And yeah, I got one and it really doubled if not tripled my sedentary time! |
I mean, it's already bad enough that today's kids spend 70% of their time with sedentary activity, only 23% with light activity (like walking from the sofa to freezer ;-), 7% with modest and only 0.6% with vigorous physical activity, wouldn't it be wise then, to rather shoot for the stars and work towards a much higher amount of vigorous activity? After all, even Hay's own study shows that only vigorous activity was associated with a reduced waist circumference and lower markers of metabolic disease (see illustration on the right).
Even if the kids don't make it to the moon, but over to the neighbor's basketball hoop or a public playground that would be a major improvement over the 'exhausting' walks from the Playstation to the fridge and back, wouldn't it?
- Pomegranate the better statin? Adding pomegranate phytosterol (β-sitosterol) and polyphenolic antioxidant (punicalagin) to a statin and reduce adipose tissue ROS production by a whopping 73%! In their most recent paper Mira Rosenblat, Nina Volkova, Michael Aviram report that the administration of Simvastatin (15 μg/ml) to macrophages in the petri dish did only only "modestly decreased macrophage reactive oxygen species (ROS)" (Rosenblat. 2012), the presence of punicalagin (15 or 30 μM) almost 'extinguished the fire' cutting back inflammation dose-dependently by another 61% or 79%.
Intriguingly, β-sitosterol alone showed had minor pro-oxidant activity, when it was administered to the J774A.1 macrophages cell line the researchers from The Lipid Research Laboratory in Haifa (Israel) were analyzing,As a regular here at the SuppVersity yo will still be aware that Pomegranate does also contain a potent plant version of CLA, called CLnA, no? Well then go back and read the full article! "the combination of simvastatin, β-sitosterol and punicalagin, clearly demonstrated a remarkable 73% reduction in ROS production."
So what's the use of the statin, then? After all the scientists also found (but rather not mention in their abstract) that the combination of β-sitosterol and punicalagin actually suppressed macrophage cholesterol synthesis as effectively as low dose Simvastin or high dose Pravastatin (Click here to read about pomegranate in the SuppVersity news) - Organo-Magnesium stops colon cancer in its tracks by inhibiting inflammation, and the findings a group of researchers from the Gifu University Graduate School report in a soon-to-be published paper are not surprising. After all many epidemiological studies studies like Folsom & Hong (2006), for example, have already shown that there is a -23% reduced risk of developing colon cancer for 55-65 year-old Swedish women in the highest vs. lowers quantile of magnesium intake. Earlier this year Wark et al. conducted a randomized trial and meta-analysis of the hitherto published studies and found:
"Our findings support the hypothesis that higher intakes of dietary magnesium are associated with lower risk of colorectal tumors. The consumption of magnesium-rich foods may be a new avenue to explore further in the search for cancer-prevention strategies." (Wark. 2012)
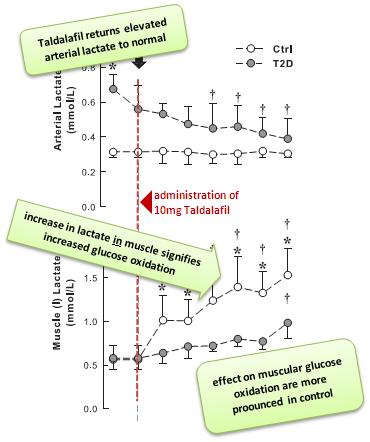
Tabs or capsules? A 2010 study has the answer to the question which form of supplemental minerals is the best for you. Roswitha Siener and her colleagues from the University of Bonn in Germany found that magnesium oxide from effervescent tablets is better absorbed than from capsules and you can be pretty sure that similar results will be found for other forms of magnesium. My advice would yet be: Save the money and just go for plain magnesium citrate powder.The meta analysis yielded 13% lower risk of colorectal adenomas and 12% lower risk of colorectal cancer for every additional 100mg of magnesium per day. This does yet not mean that by eating pounds of magnesium you could render yourself 'cancer proof', but it is good evidence to make sure to get at least the into the 380-500mg range. And if you want to supplement, you really won't need the organ-magnesium Kuno et al. produced by mixing magnesium oxide (0.22 g), citric acid (0.55 g), malic acid (0.55 g), and glycine (0.22 g) - unless you can't tolerate it, cheap magnesium citrate will do just as well. - Taldalafil for insulin resistant and healthy post-menopausal women?! (Murdolo. 2012) A group of European scientists have found that the administration of 10mg of Taldalfil (the notorious PDE-5 inhibitor in Cialis) to both diabetic and healthy controls led to
- an increase in permeability surface area product for glucose , and
- skeletal muscle interstitial lactate levels r
Based on these findings, Guiseppe Murdolo and his colleagues argue that the results would suggest that acute Tadalafil administration can increase the capillary recruitment and nonoxidative glucose metabolism, without having consistent effects on forearm blood flow and regional lipolytic rate. However...
Figure 1: Effects of 10mg of Taldalafil on arterial and intramuscular lactate concentration (Murdolo. 2012). The increase in intramuscular glucose oxidation (evidenced by the lactate that is generated during this process) could even be of interest to healthy women (and men?). "[...] notwithstanding the lack of measurable changes on forearm glucose uptake, the microvascular response to tadalafil emerged as an independent predictor of muscle glucose disposal in both T2D patients and insulin-sensitive controls."
Well, and if those effects don't reach statistical significance, maybe 'others' will. After all a 2003 study by Caruso et al. suggests that Taldalafil can also increase "the frequency of sexual fantasies and of sexual intercourse, and enjoyment" (Caruso. 2003) in a group of 53 pre-menopausal women (age 22–28) years affected by arousal disorders. Maybe we should simply put Taldalfil into the drinking... ah, I am just kidding ;-) - Finally! Scientists determine 'exactly'*rofl* how much more muscle you can gain with supplemental protein (Cermak. 2012). I hope I do not have to point you towards the irony in the headline of this On Short Notice item. If this ain't your first visit to the SuppVersity you should by now be aware that calculations like add 1g of protein per day and gain x-amounts of lean muscle mass per month, year or whatever timespan are nonsensical and will provide, if anything, a very general orientation.
That said, it is still interesting to see the actual results Naomi M Cermak et al.'s quantitative meta-analysis of 22 studies, of which 77% were conducted with untrained individuals (64% with young trainees) produced. Most studies, which had a duration of 6-24 weeks (median: 12 weeks), used 3-5 x whole body workouts / splits coupled with milk (mostly whey) protein supplementation in amounts that ranged from 10g to 106g - keep that in mind when you think about how 'exact' the following figures can actually be:
Fat free and fat mass - Compared with the placebo, protein supplementation significantly augmented the gain in FFM during prolonged resistance-type exercise training (weighted mean difference: 0.69 kg). A subgroup analysis for age showed that protein supplementation was beneficial for both the young and the old trainees, but that the total effect size in terms of fat free mass gains were ~1.7x higher in the young subject (+0.81 kg) than in the older ones (+0.48 kg;) subjects.
Size-wise and even more so strength-wise Arnold could still benefit from a protein shake after a workout. When it comes to the increases in type I and type II fiber CSA, his age could however put a spoke in his wheel.
What I find particularly surprising is that the subgroup analysis also revealed that training status had no significant and what's more, if anything a beneficial effect on the effect sizes in the young untrained (+0.75 kg) and trained subjects (+0.98 kg), respectively.
As far as fat loss is concerned the scientists did not record any statistical significant differences compared to placebo and that despite the fact that the placebo in most of the 22 studies was a sugary carbohydrate drink.- Muscle fiber cross sectional area - As the gains in lean mass already suggest, the cross sectional area (CSA) of the muscle fibers increased: By ~ 212µm² in the type I fibers and 291µm² in type II fibers. Unfortunately, both the increases in type I and type II fibers were statistically significant only in the young trainees.
- 1-RM Strength - The performance for the one-rep maximum (1RM) on the leg press improved across the board (+13.5kg more than in placebo) and that did work almost equally well for younger (+14.4kg) and older trainees (+13.1kg).


References:
- Caruso S, Intelisano G, Lupo L, Agnello C. Premenopausal women affected by sexual arousal disorder treated with sildenafil: a double-blind, cross-over, placebo-controlled study. BJOG. 2001 Jun;108(6):623-8.
- Cermak NM, Res PT, de Groot LC, Saris WH, van Loon LJ. Protein supplementation augments the adaptive response of skeletal muscle to resistance-type exercise training: a meta-analysis. Am J Clin Nutr. 2012 Nov 7.
- Folsom AR, Hong CP. Magnesium intake and reduced risk of colon cancer in a prospective study of women. Am J Epidemiol. 2006 Feb 1;163(3):232-5.
- Hay J, Maximova K, Durksen A, Carson V, Rinaldi RL, Torrance B, Ball GD, Majumdar SR, Plotnikoff RC, Veugelers P, Boulé NG, Wozny P, McCargar L, Downs S, Lewanczuk R, McGavock J. Physical Activity Intensity and Cardiometabolic Risk in Youth. Arch Pediatr Adolesc Med. 2012 Sep 10:1-8. doi: 10.1001/archpediatrics.2012.1028.
- Kuno T, Hatano Y, Tomita H, Hara A, Hirose Y, Hirata A, Mori H, Terasaki M, Masuda S, Tanaka T. Organo-Magnesium Suppresses Inflammation-Associated Colon Carcinogenesis in Male Crj: CD-1 Mice. Carcinogenesis. 2012 Nov 3.
- Murdolo G, Sjöstrand M, Strindberg L, Lönnroth P, Jansson PA. The Selective Phosphodiesterase-5 Inhibitor Tadalafil Induces Microvascular and Metabolic Effects in Type 2 Diabetic Postmenopausal Females. J Clin Endocrinol Metab. 2012 Nov 1.
- Rosenblat M, Volkova N, Aviram M. Pomegranate phytosterol (β-sitosterol) and polyphenolic antioxidant (punicalagin) addition to statin, significantly protected against macrophage foam cells formation. Atherosclerosis. Available online 31 October 2012.
- Siener R, Jahnen A, Hesse A. Bioavailability of magnesium from different pharmaceutical formulations. Urol Res. 2011 Apr;39(2):123-7.
- Wark PA, Lau R, Norat T, Kampman E. Magnesium intake and colorectal tumor risk: a case-control study and meta-analysis. Am J Clin Nutr. 2012 Sep;96(3):622-31. doi: 10.3945/ajcn.111.030924. Epub 2012 Aug 1.