 |
| I usually rant against pizza and beer, but once the athlete triad has struck, they can be an occasional part of the "healing protocol". |
Which endocrine factors are figuring, here?
Instead of overwhelming you with the details right from the start, I decided to compile a list based on a cross-section of the dozens of articles I have read in the course of my eventually futile quest for a single definitive answer to the question, "Which hormonal or metabolic consequence of restrictive eating and excessive training is to blame for the fatigue, the low sex hormones concentration,the bone resorption, the anemia, the absence of menses / lack of libido, the performance decreases and the whole string of pathological features, we have explored in the last installment?"
"Refeeding is not an option, because you will only become fat!" FALSE! Yet another myth without substantial scientific foundation that probably arises from the disturbed self-perception of those affected by AT and AN. In fact, the fat stores are the last thing that will be restored (Golden. 2004). This is probably also one of the reasons why "refeeding" often does not appear to work, because the basal energy requirements will increase with every pound of lean tissue you add back to your frame, so that athletes suffering from the "triad" will have to continuously increase their energy consumption. Unfortunately, most athletes will fail to do the former (also because exercise & stress can blunt hunger) and instead react with an increase in workout intensity, now that they are finally able to work out, again. This, in turn, will restore or even exacerbate the energy deficit and thus worsen not improve their physiological problems, even if their scale shows that they have already gained 5-10kg. If you take a look at figure 1 you will also realize that, at least in women, a baseline level of total (not relative!) body fat appears to be necessary to maintain regular menses (in men to maintain normal total testosterone & SHBG, but not so much free testosterone levels or reproductive function).
- low luteinizing levels are unquestionably among the elemental features and causally responsible for the occurance of menstrual disorders / lack of libido and the correspondingly low estrogen and testosterone levels in women and men
- TSH levels are not a valid / reliable indicator for the presence of absence of AT, because they can be both slightly increased or normal in the presence of low T4 and low T3 levels, as - and this is far more often the case - TSH can be low despite low free thyroid hormone levels (usually in the presence of a low T3/rt3 ratio; if anything this would be a good indicator of beginning or full-blown AT)
- the circadian cortisol rhythm is whacked in men and women, alike; characteristic are the absence of an appropriate cortisol spike in the morning as well as the normal decline in cortisol levels in the course of the day; metaphorically speaking, as the athletes triad progresses, the "mountain range" turns into mesa and eventually into a plane lowland
- the quartet of (mostly) sub-clinical hypogylcemia, low insulin, extreme high / or totally blunted insulin sensitivity, low IGF-1 and high catecholamine levels cannot be seen in isolation, most detrimental are yet probably the first and last of these four glucose-related players in the AT concert, as the former entails the constant risk to run out of "brain fuel" (in the absence of alternative fuel sources) and can - in the absence of adequate corticosteroid expression - become potentially life-threatening and the latter, i.e. low IGF-1 levels and very low IGF-1 to IGF1 binding protein 4 being one of the, if not the central factor involved in the the long-term physical decline of muscle, bone, organ and even brain mass.
- tapping into its energy stores in form of body fat, muscle and organ mass, the insulating fat around nerves and organs, etc.,
- continuously decreasing its metabolic activity (esp. thyroid metabolism),
- shutting down non-vital, but energy-intensive (e.g. immune and reproductive system) bodily functions, to prioritize short term survival of the individual over long-term survival and the conservation of the species
And what about leptin, ghrelin, adiponectin ... ?
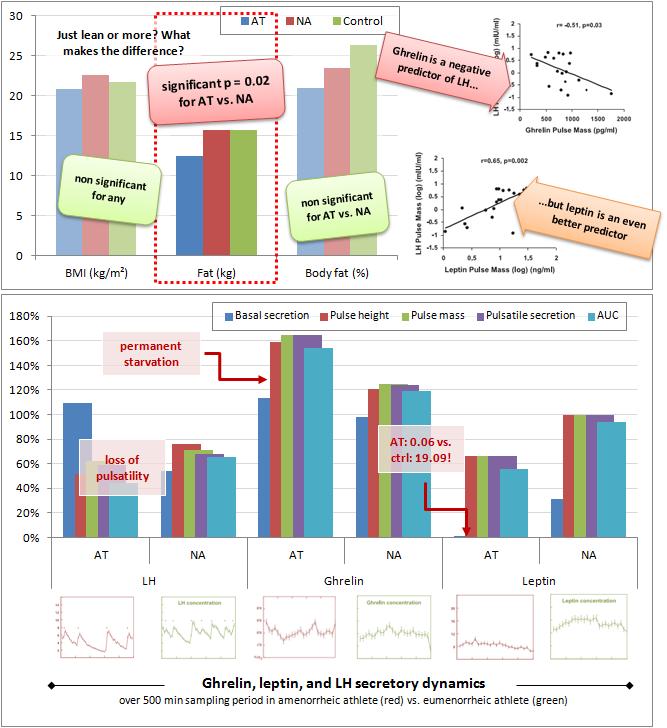 |
| Figure 1: In female athletes, only total fat mass, not body fat % or BMI are associated w/ AT (here identified by amenorrhea; top, left); the correspondingly low pulsatile (not baseline, see lower left) of LH correlate negatively with ghrelin and positively with leptin (top, right); while LH and leptin show a lack of pulsality, the ghrelin levels are not simply elevated, they also have a higher pulse size, amplitude and total polsatile secretion compared to control and eumenorrhetic athletes (bottom; LH, ghrelin, leptin expressed relative to non-athletic control; based on Ackerman. 2012) |
And as if that alone would not already make it difficult enough to separate cause and effect, it does actually appear likely that the order may even be reversed over time - not unlike the chicken that will hatch and eventually lay an egg.
As discussed in the last installment, the combination of over-exercising and fasting, which may at time-point T0 actually have been the root cause of the problem will often turn into a strategy to stave off the impeding total breakdown. It becomes sort of a conditioned response to the constant starvation, which will then no longer manifest itself in the form of hunger, but as anxiety and an almost compulsive urge to exercise (this is particularly well-established for anorexics; Teufel. 2008). And while the latter can be motivated by the desire to increase athletic performance and/or lose even more body fat, it does have a very real, often under-appreciated, physiological underpinning.
If you like, you could argue that the urge of the starved athlete to exercise is yet another "evolutionary conserved" automatism that mirrors the well-known food-seeking behavior rodents display in periods of food deprivation and in response to the stimulatory effects of ghrelin on the orexin neurons in the brain (Yamanaka. 2003).
From ghrelin to growth hormone to IGF-1 and back
At the same time, the combination of exercise, low triglyceride, low free fatty acid and exuberant levels of the "hunger hormone" ghrelin leads to an overexpression of growth hormone (Scacci. 2003), subsequent increases in adiponectin (Wölfing. 2008), which will in turn decrease progesterone and androstenedione production and LH receptor expression in ovarian cells (Lagaly. 2008) and GnRH and LH release in the pituitary (Rodriguez-Pacheco. 2007; Lu. 2008). The surprisingly high adiponectin levels (surprisingly in view of the often dangerously low levels of adipokine producing body fat) will further increase the borderline pathological insulin sensitivity and thus lower the already rock bottom blood glucose and basal, as well as (post-)prandial insulin levels even further.
 |
| Figure 2: Illustration of the self-perpetuating vicious cycle of the athlete's triad (AT) |
* in view of the insulinogenic effects of whey and the pro-IGF-1 effects of casein (Hoppe. 2009), and the anti-catabolic effects of CLA & omega-3 you should - if by any means possible - incorporate dairy products from preferably grass fed dairy (butter, milk, cheese, yoghurt, quark / curd cheese, fermented dairy and if you want protein powders) in your diet regularly, better daily.
- adequate and continuous energy supply to control ghrelin levels and help stabilize blood sugar (and thus glucocorticoid) levels and restore normal leptin and adiponectin expression,
- increased low GI (to avoid reactive hypoglycemia) carbohydrate and protein intakes to normalize glucose levels, suppress ghrelin, increase insulin and IGF-1 levels* (Foster-Schubert. 2008; suggested read: "Carbohydrate Shortage in Paleo Land"),
- balanced intakes of all types of natural fats, with an emphasis on long-chain PUFAs from food including a reasonable amount of "bad" omega-6 fatty acids and w/out fish oil or other omega-3 supplements, which would further blunt the already compromised glucocorticoid response and the leptin secretion (Kratz. 2002; suggested read "Omega-3 and Low Cortisol"), and
- profound reductions in training volume to lower GH, cortisol, catecholamin and energy requirements and a (temporary) reorientation towards low volume strength training that will help increase bone density and IGF-1 expression (Davee. 1990)
 |
| Figure 3: Development of BMI (blue), leptin (red), adiponectin (green) levels in 8 female adolescent malnourished AN patients (based on Modan-Moses. 2007) |
In view of the fact that other studies have shown that this increase in weight, which must not be confused with a mere increase in adiposity, i.e. body fat percentage (go back to figure 1 if you already forgot that the absolute not the relative fat mass counts and please remember that the latter includes the fat in the myelin sheaths of your nerves, the protective fat around the organs, the fat in your brain etc.), does help with the normalization of both insulin and ghrelin (Otto. 2001), growth hormone and IGF-1 (Argente. 1997) and is in some cases even sufficient to restore most of the endocrine abnormalities (Scheid. 2010), many of the lessons we will learn in the next (and according to my current plans last ;-) installment can also be applied to a lean bulk - and that goes irrespective of your gender and your whether or not you have already fallen victim to the athlete triad!
References
- Ackerman KE, Slusarz K, Guereca G, Pierce L, Slattery M, Mendes N, Herzog DB, Misra M. Higher ghrelin and lower leptin secretion are associated with lower LH secretion in young amenorrheic athletes compared with eumenorrheic athletes and controls. Am J Physiol Endocrinol Metab. 2012 Apr 1;302(7):E800-6.
- Argente J, Caballo N, Barrios V, Muñoz MT, Pozo J, Chowen JA, Morandé G, Hernández M. Multiple endocrine abnormalities of the growth hormone and insulin-like growth factor axis in patients with anorexia nervosa: effect of short- and long-term weight recuperation. J Clin Endocrinol Metab. 1997 Jul;82(7):2084-92.
- Beals KA, Manore MM. Disorders of the female athlete triad among collegiate athletes. Int J Sport Nutr Exerc Metab. 2002 Sep;12(3):281-93.
- Boag F, Weerakoon J, Ginsburg J, Havard CW, Dandona P. Diminished creatinine clearance in anorexia nervosa: reversal with weight gain. J Clin Pathol. 1985 Jan;38(1):60-3.
- Böni-Schnetzler M, Hauri C, Zapf J. Leptin is suppressed during infusion of recombinant human insulin-like growth factor I (rhIGF I) in normal rats. Diabetologia. 1999 Feb;42(2):160-6.
- Caspar-Bauguil S, Montastier E, Galinon F, Frisch-Benarous D, Salvayre R, Ritz P. Anorexia nervosa patients display a deficit in membrane long chain poly-unsaturated fatty acids. Clin Nutr. 2012 Jun;31(3):386-90.
- Davee AM, Rosen CJ, Adler RA. Exercise patterns and trabecular bone density in college women. J Bone Miner Res. 1990 Mar;5(3):245-50.
- Di Carlo C, Palomba S, De Fazio M, Gianturco M, Armellino M, Nappi C. Hypogonadotropic hypogonadism in obese women after biliopancreatic diversion. Fertil Steril. 1999 Nov;72(5):905-9.
- Di Luigi L. Does the high performance athlete need hormone replacement? Endocrine Abstracts. 2012; 29: 35.1
- Foster-Schubert KE, Overduin J, Prudom CE, Liu J, Callahan HS, Gaylinn BD, Thorner MO, Cummings DE. Acyl and total ghrelin are suppressed strongly by ingested proteins, weakly by lipids, and biphasically by carbohydrates. J Clin Endocrinol Metab. 2008 May;93(5):1971-9.
- Figueiro MG, Plitnick B, Rea MS. Light Modulates Leptin and Ghrelin in Sleep-Restricted Adults. International Journal of Endocrinology. 2012, Article ID 530726.
- Golden NH, Meyer W. Nutritional rehabilitation of anorexia nervosa. Goals and dangers. Int J Adolesc Med Health. 2004 Apr-Jun;16(2):131-44.
- Hernández M, Argente J, Navarro A, Caballo N, Barrios V, Hervás F, Polanco I. Growth in malnutrition related to gastrointestinal diseases: coeliac disease. Horm Res. 1992;38 Suppl 1:79-84.
- Hobart J, Smucker D. The Female Athlete Triad. Fam Physician 2000; 61:3357-64,3367.
- Hoppe C, Mølgaard C, Dalum C, Vaag A, Michaelsen KF. Differential effects of casein versus whey on fasting plasma levels of insulin, IGF-1 and IGF-1/IGFBP-3: results from a randomized 7-day supplementation study in prepubertal boys. Eur J Clin Nutr. 2009 Sep;63(9):1076-83.
- Khan KM, Liu-Ambrose T, Sran MM, Ashe MC, Donaldson MG, Wark JD. New criteria for female athlete triad syndrome? As osteoporosis is rare, should osteopenia be among the criteria for defining the female athlete triad syndrome? Br J Sports Med. 2002 Feb;36(1):10-3.
- Klok MD, Jakobsdottir S, Drent ML. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: a review. Obes Rev. 2007 Jan;8(1):21-34.
- Kratz M, von Eckardstein A, Fobker M, Buyken A, Posny N, Schulte H, Assmann G, Wahrburg U. The impact of dietary fat composition on serum leptin concentrations in healthy nonobese men and women. J Clin Endocrinol Metab. 2002 Nov;87(11):5008-14.
- Lagaly DV, Aad PY, Grado-Ahuir JA, Hulsey LB, Spicer LJ. Role of adiponectin in regulating ovarian theca and granulosa cell function. Mol Cell Endocrinol. 2008 Mar 12;284(1-2):38-45.
- Leibel RL, Rosenbaum M, Hirsch J. Changes in energy expenditure resulting from altered body weight. N Engl J Med. 1995 Mar 9;332(10):621-8. Erratum in: N Engl J Med 1995 Aug 10;333(6):399.
- Loucks AB, Verdun M, Heath EM. Low energy availability, not stress of exercise, alters LH pulsatility in exercising women. J Appl Physiol. 1998 Jan;84(1):37-46.
- Loucks AB. Energy availability, not body fatness, regulates reproductive function in women. Exerc Sport Sci Rev. 2003 Jul;31(3):144-8.
- Lu M, Tang Q, Olefsky JM, Mellon PL, Webster NJ. Adiponectin activates adenosine monophosphate-activated protein kinase and decreases luteinizing hormone secretion in LbetaT2 gonadotropes. Mol Endocrinol. 2008 Mar;22(3):760-71. Epub 2007 Nov 15.
- Manore MM. Dietary recommendations and athletic menstrual dysfunction. Sports Med. 2002;32(14):887-901.
- Mikos AE, McDowell BD, Moser DJ, Bayless JD, Bowers WA, Andersen AE, Paulsen JS. Stability of neuropsychological performance in anorexia nervosa. Ann Clin Psychiatry. 2008 Jan-Mar;20(1):9-13.
- Miller SM, Kukuljan S, Turner AI, van der Pligt P, Ducher G. Energy deficiency, menstrual disturbances, and low bone mass: what do exercising Australian women know about the female athlete triad? Int J Sport Nutr Exerc Metab. 2012 Apr;22(2):131-8.
- Modan-Moses D, Stein D, Pariente C, Yaroslavsky A, Ram A, Faigin M, Loewenthal R, Yissachar E, Hemi R, Kanety H. Modulation of adiponectin and leptin during refeeding of female anorexia nervosa patients. J Clin Endocrinol Metab. 2007 May;92(5):1843-7. Epub 2007 Feb 27.
- Mont L, Castro J, Herreros B, Paré C, Azqueta M, Magriña J, Puig J, Toro J, Brugada J. Reversibility of cardiac abnormalities in adolescents with anorexia nervosa after weight recovery. J Am Acad Child Adolesc Psychiatry. 2003 Jul;42(7):808-13.
- Murdolo G, Lucidi P, Di Loreto C, Parlanti N, De Cicco A, Fatone C, Fanelli CG, Bolli GB, Santeusanio F, De Feo P. Insulin is required for prandial ghrelin suppression in humans. Diabetes. 2003 Dec;52(12):2923-7.
- NCAA® Sports Sponsorship and Participation Rates Report • 1981-82 – 2010-11.
- Orlandi E, Boselli P, Covezzi R, Bonaccorsi G, Guaraldi GP. Reversal of bone marrow hypoplasia in anorexia nervosa: case report. Int J Eat Disord. 2000 May;27(4):480-2.
- Ott V, Fasshauer M, Dalski A, Meier B, Perwitz N, Klein HH, Tschöp M, Klein J. Direct peripheral effects of ghrelin include suppression of adiponectin expression. Horm Metab Res. 2002 Nov-Dec;34(11-12):640-5.
- Otto B, Cuntz U, Fruehauf E, Wawarta R, Folwaczny C, Riepl RL, Heiman ML, Lehnert P, Fichter M, Tschöp M. Weight gain decreases elevated plasma ghrelin concentrations of patients with anorexia nervosa. Eur J Endocrinol. 2001 Nov;145(5):669-73.
- Rguibi M, Belahsen R. Body size preferences and sociocultural influences on attitudes towards obesity among Moroccan Sahraoui women. Body Image. 2006 Dec;3(4):395-400. Epub 2006 Sep 7.
- Rodriguez-Pacheco F, Martinez-Fuentes AJ, Tovar S, Pinilla L, Tena-Sempere M, Dieguez C, Castaño JP, Malagon MM. Regulation of pituitary cell function by adiponectin. Endocrinology. 2007 Jan;148(1):401-10.
- Scacchi M, Ida Pincelli A, Cavagnini F. Nutritional status in the neuroendocrine control of growth hormone secretion: the model of anorexia nervosa. Front Neuroendocrinol. 2003 Jul;24(3):200-24.
- Scheid JL, De Souza MJ. Menstrual irregularities and energy deficiency in physically active women: the role of ghrelin, PYY and adipocytokines. Med Sport Sci. 2010;55:82-102.
- Schtscherbyna A, Barreto T, de Oliveira FP; Luiz RR, de Abreu Soares RR, Gonçalves Ribeiro B. Age of onset training but not body composition is crucial in menstrual dysfunction in adolescent competitive swimmers. Rev Bras Med Esport. May/June 2012; 18(3).
- Steinberg SE, Nasraway S, Peterson L. Reversal of severe serous atrophy of the bone marrow in anorexia nervosa. JPEN J Parenter Enteral Nutr. 1987 Jul-Aug;11(4):422-3.
- Skarda ST, Burge MR. Prospective evaluation of risk factors for exercise-induced hypogonadism in male runners. West J Med. 1998 Jul;169(1):9-12.
- Sundgot-Borgen J. [Physical activity and reproductive health]. Tidsskr Nor Laegeforen. 2000 Nov 20;120(28):3447-51.
- Teufel M, Zipfel S, Herpertz S, Zwaan M. (ed.). Handbuch Essstörungen und Adipositas. Springer Berlin Heidelberg. 2008.
- Williams NI, Helmreich DL, Parfitt DB, Caston-Balderrama A, Cameron JL. Evidence for a causal role of low energy availability in the induction of menstrual cycle disturbances during strenuous exercise training. J Clin Endocrinol Metab. 2001 Nov;86(11):5184-93.
- Wölfing B, Neumeier M, Buechler C, Aslanidis C, Schölmerich J, Schäffler A. Interfering effects of insulin, growth hormone and glucose on adipokine secretion. Exp Clin Endocrinol Diabetes. 2008 Jan;116(1):47-52.
- Yamanaka A, Beuckmann CT, Willie JT, Hara J, Tsujino N, Mieda M, Tominaga M, Yagami K, Sugiyama F, Goto K, Yanagisawa M, Sakurai T. Hypothalamic orexin neurons regulate arousal according to energy balance in mice. Neuron. 2003 Jun 5;38(5):701-13.