 |
| Image 1: The person in the middle was probably once morbidly obese. How I know? Lower body adipose tissue sticks. |
The fat you gain today, will not be gone tomorrow!
In the scientific version of "from fit2fat2fit" (click here to watch the ABC report on the "experiment"), Prachi Singh and his colleagues from the Mayo Clinic in Rochester, UK, fed 23 volunteers (15 men and 8 women; BMI 23.6 6kg/m², mean age 30y), who were sedentary, but normal-weight and free of chronic disease, standardized diets with a macronutrient composition of 20% protein, 40% carbs and 40% fat. In addition each of the participants, who were weighed at least 5x per week had to eat 1-3 of the following snacks
- ice-cream shake (402 kcal),
- chocolate bars (a king-size Snickers bar, 510 kcal), or
- an energy drink (Boost Plus, 360 kcal/8 oz)
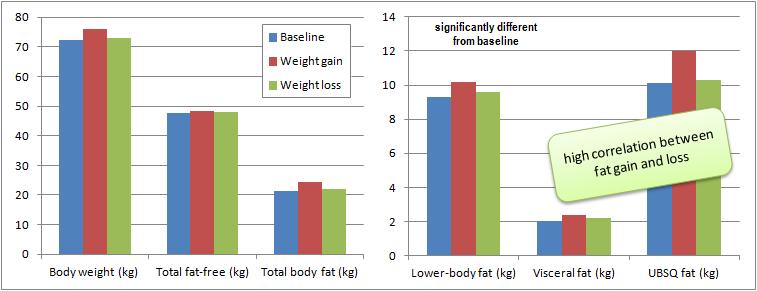 |
| Figure 1: Body composition and fat depot weight at baseline and after weight gain and loss (based on Singh. 2012) |
 |
| Figure 2: Correlation of changes in lower-body fat mass and femoral fat cell size (men: squares, women: circles; Singh. 2012) |
Faster in faster out ain't the whole explanation, though.
 |
| Image 2: You can ask any bodybuilder, a six-pack is easier to get than striated glutes & hamstrings. And the difference between upper - and lower body fat storage could well explain this phenomenon! |
- upper body subcutaneous fat mass increases (mainly) by cellular hypertrophy
- lower body subcutaneous fat mass increases (mainly) by cellular hyperplasia
Hypertophy vs. hyperplasia - the latter sticks!
In fact previous research suggests that as soon as the storage ability of the individual fat cells is exceeded, hyperplasia becomes the predominant way to increase the bodies fat storage capacities (usually this is also when the overflowing existing adipose tissue stores begin to "burn down" the house by releasing copious amounts of inflammatory cytokines; cf. Skurk. 2007). Consequently,
[a]fter weight loss, obese people have smaller adipocytes than do people with a similar percentage of body fat and stable weight [though] it is unknown whether those obese adults had more adipocytes before they became obese [...] evidence has suggested that postobese adults have a larger number of fat cells, which could be a long-term consequence of adult weight gain on adipose tissue cellularity. (Singh 2012)And in fact, these changes in "adipose tissue cellularity" became obvious in the study at hand after no more than 8 weeks of weight gain and loss - life long body fat accumulation or weight gain in the double digit range may not even be necessary...
Limitations of the study: Taken on it's own the Singh study does yet fail to prove the hypothesis that weight gain is associated with increases in fat cell number while weight loss is not, simply because the scientists did take biopsies only at the end of the study - in my eyes a major design flaw, irrespective of the fact, whether the data they would have elucidated would have been "statistically non-significant", as they point out. I did therefore decide against plotting the respective data on adipocyte size and number because without appropriate knowledge of where the subjects were coming from it is worthless anyway.
In this context, it is also noteworthy that the amount of leptin that's released by a given fat cell appears to (non-linearly!) increase with it's size. Against that background the "adipocyte abundance" (many now almost empty fat cells with a very low leptin secretion) in formerly obese subjects could even explain why most of them are having a very hard time to keep the weight off, let alone shed those pounds that still cover their abs, buttocks, etc. After all, on the individual cell level, their body fat stores are in fact almost empty - regardless of the fact that these people still carry 20+ more pounds of body fat on their frame than someone who has not gotten obese in the first place.Bottom line: NEVER go from fit2fat!
 |
| Video 1 (click here to watch): Don't do the "Drew Manning" - making money and becoming famous with being fat is not going to work out another time - after all, Ozzy has already had it on the show... well, maybe if you used Ozzy's Rasberry product (see previous post) to shed the weight again ;-) |
There are studies that suggest that supplements like CLA could help accelerate this process (Tsuboyama-Kasaoka. 2000). Unfortunately, the data comes from rodent studies, many human trials on the other hand did not elicit any beneficial results, in parts certainly due to lower dosages, which are however a safety measure to prevent side effects such as the profound insulin resistance and hyperinsulinemia Tsuboyma-Kasoaka et al. observed in their study. It appears only logical that the latter would be a direct consequence of the combination of triglyceride release profoundly reduced leptin levels in response to the sudden death of the fat cells, which was in fact so pronounced that the scientists do speak of "lipodystrophy", a medical condition characterized by abnormal or degenerative conditions of the body's adipose tissue.
In the end, the only feasible option left appears - once again - to turn your life inside out and wait until the pendulum will have swung back into the right direction.
References:
- Della-Fera MA, Qian H, Baile CA. Adipocyte apoptosis in the regulation of body fat mass by leptin. Diabetes Obes Metab. 2001 Oct;3(5):299-310.
- Dilzer A, Park Y. Implication of conjugated linoleic acid (CLA) in human health. Crit Rev Food Sci Nutr. 2012;52(6):488-513.
- Guo Z, Johnson CM, Jensen MD. Regional lipolytic responses to isoproterenol in women. Am J Physiol 1997;273:E108–12.
- Jensen MD, Sarr MG, Dumesic DA, Southorn PA, Levine JA. Regional uptake of meal fatty acids in humans. Am J Physiol Endocrinol Metab 2003;285:E1282–8.
- Löfgren P, Andersson I, Adolfsson B, Leijonhufvud B, Hertel K, Hoffstedt J, Arner P. Long-term prospective and controlled studies demonstrate adipose tissue hypercellularity and relative leptin deficiency in the postobese state. J Clin Endocrinol Metab 2005;90:6207–13.
- Marin P, Rebuffe-Scrive M, Bjorntorp P. Uptake of triglyceride fatty acids in adipose tissue in vivo in man. Eur J Clin Invest 1990;20:158–65.
- Martin ML, Jensen MD. Effects of body fat distribution on regional lipolysis in obesity. J Clin Invest 1991;88:609–13.
- Nielsen S, Guo ZK, Johnson CM, Hensrud DD, Jensen MD. Splanchnic lipolysis in human obesity. J Clin Invest 2004;113:1582–8.
- Skurk T, Alberti-Huber C, Herder C, Hauner H. Relationship between adipocyte size and adipokine expression and secretion. J Clin Endocrinol Metab. 2007
- Spalding KL, Arner E, Westermark PO, Bernard S, Buchholz BA, Bergmann O, Blomqvist L, Hoffstedt J, Naslund E, Britton T, et al. Dynamics of fat cell turnover in humans. Nature 2008;453:783–7
- Tchoukalova YD, Votruba SB, Tchkonia T, Giorgadze N, Kirkland JL, Jensen MD. Regional differences in cellular mechanisms of adipose tissue gain with overfeeding. Proc Natl Acad Sci USA 2010;107: 18226–31.
- Tsuboyama-Kasaoka N, Takahashi M, Tanemura K, Kim HJ, Tange T, Okuyama H, Kasai M, Ikemoto S, Ezaki O. Conjugated linoleic acid supplementation reduces adipose tissue by apoptosis and develops lipodystrophy in mice. Diabetes. 2000 Sep;49(9):1534-42.